CASE : A 60 year old women is noted to have 2 cm of mass in her left breast. The patient doctor recommends her core needle biopsy. Tissue analysis by the pathologist under the microscope reveals the Intraductal carcinoma or Ductal Carcinoma insitu. The Surgeon suggested the patient to have surgery to remove the primary beast mass along with the affected lymph nodes if found.
You Can Download My detail presentation on ” INDTRADUCTAL CARCINOMA “/ DCIS .PPT by Clicking here
1. OVERVIEW OF THE CASE & IMPORTANCE OF EARLY DIAGNOSIS
Diagnosis:
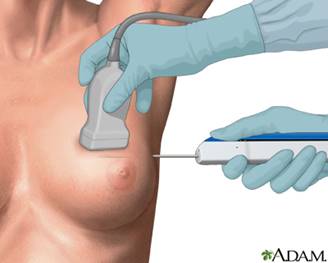
Imaging: Mammogram and ultrasound confirmed suspicious mass.
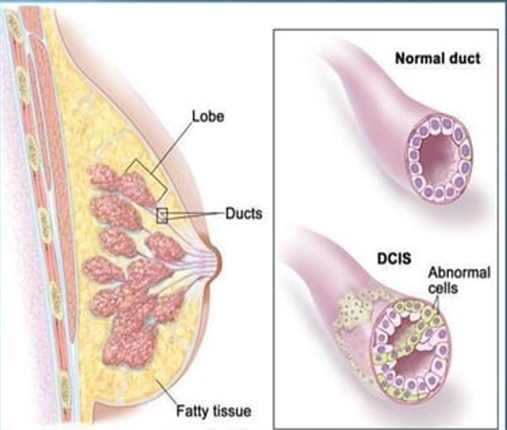
Biopsy: Core needle biopsy showed intraductal carcinoma (DCIS).
Surgical Treatment:
– Wide excision (lumpectomy) of the breast mass.
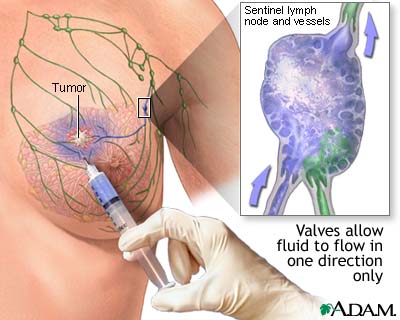
– Sentinel lymph node biopsy and removal.
Pathology Results :
– Confirmed DCIS ( Ductal Carcinoma In Situ / Intraductal Carcinoma )
– Clear surgical margins.
– Cancer in lymph node ( sentinel lymph node found in Level I axillary lymph nodes).
Postoperative Management:
– Regular follow-up exams and imaging.
– Possible additional treatments like radiation or hormone therapy based on further tests (ER, PR, HER2 status).
Prognosis: ( Outcome )
– Early detection leads to a favorable outcome.
– Continued monitoring to check for recurrence.
Importance of early detection and diagnosis in Breast Cancer
Early detection and diagnosis of breast cancer are vital for improving survival rates, reducing the need for aggressive treatments, enhancing treatment efficacy, lowering healthcare costs, and addressing healthcare disparities.
Regular screening and awareness are key components in the fight against breast cancer, empowering individuals to take proactive steps in managing their health.
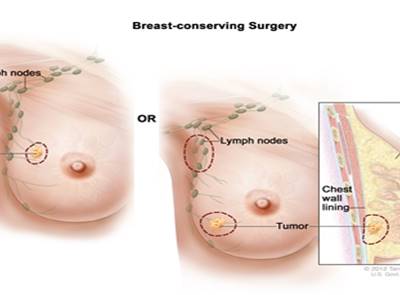
2. TREATMENT OF THE BREAST CANCER IN THIS CASE
Wide Local Excision (Lumpectomy):
During the surgery, the surgeon makes an incision over the breast and carefully removes the tumor along with a surrounding margin of normal tissue. The amount of tissue removed ensures that all cancer cells are excised, reducing the risk of recurrence.
Sentinel Lymph Node Biopsy (was done in this case):
In this case, a sentinel lymph node biopsy was performed during the same procedure to check if cancer cells have spread to nearby lymph nodes and was removed.
LET US KNOW WHAT IS INTRADUCTAL CARCINOMA / DCIS – BREAST CANCER
Intraductal carcinoma / Ductal carcinoma insitu is a early form of breast cancer in which abnormal cells are developed in the lining of the milk duct in the breast but mostly in initial stage it does not spread out of the duct. It is detected by using the Mammography , Ultrasound and further Core needle biopsy is performed for the confirmation. It is usually treated by surgery and radiation and hormone therapy after surgery.
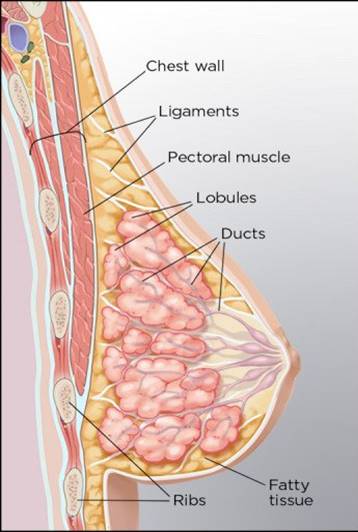
ANATOMY OF BREAST
The breast is a glandular organ located in the superior compartment of the pectoral region (second rib to the sixth rib) , made up of mammary glands, ducts, and connective tissue. These are primarily responsible for producing milk.
0. Location :
– Rests on deep fascia of the pectoralis major muscle.
– Separated by the retromammary space, allowing movement.
1. Mammary Glands:
– Modified sweat glands in the superficial fascia.
– Located in front of the pectoral muscles.
2. Ducts and Lobules:
– Form 15 to 20 lactiferous ducts per breast.
– Open onto the nipple, which is surrounded by the areola.
3. Connective Tissue Stroma:
– Forms suspensory ligaments (Cooper’s ligaments) that support the breast.
– Tension on these ligaments by carcinoma can cause skin pitting.
4. Fat Composition :
– Breasts in non-lactating women consist mainly of fat.
– More glandular tissue is present in lactating women.
5. Base of the Breast :
– Extends vertically from the second to sixth ribs.
– Horizontally from the sternum to the midaxillary line.
6. Clinical Implications :
– Important for breast self-examination and clinical breast exams.
– Understanding anatomy aids in detection and management of breast conditions, including carcinoma.
BLOOD VESSELS SUPPLYING BREAST
The breast is related to the thoracic wall and to structures associated with the upper limb; therefore, vascular supply and drainage can occur by multiple routes:
laterally, vessels from the axillary artery—superior thoracic, thoraco-acromial, lateral thoracic, and subscapular arteries;
medially, branches from the internal thoracic artery;
the second to fourth intercostal arteries via branches that perforate the thoracic wall and overlying muscle.
Veins draining the breast run parallel to the arteries and ultimately drain into the axillary, internal thoracic, and intercostal veins.
INNERVATIONS OF THE BREAST
Innervation of the breast refers to the supply of nerves to the breast tissue, which provides both sensory and autonomic (involuntary) functions
Anterior and Lateral Cutaneous Branches of the Intercostal Nerves (T2-T6)
Supraclavicular Nerves (C3-C4)
Lymph nodes draining Breast
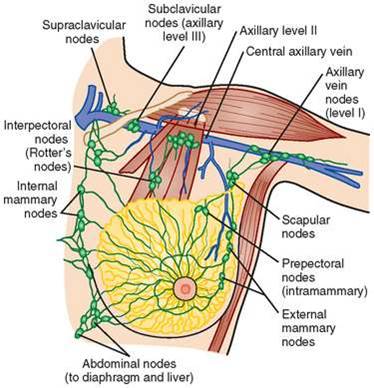
1. Axillary Lymph Nodes
These are the primary lymph nodes draining the breast and are divded into three levels.
2. Internal Mammary (Parasternal) Lymph Nodes
Located along the internal mammary vessels, near the sternum. Receive drainage from the medial portions of the breast.
3. Supraclavicular Lymph Nodes
Located above the clavicle, near the neck.
Can receive drainage from the axillary lymph nodes and indicate more advanced spread of breast cancer when involved.
ANATOMICAL STRUCTURE DEFINING THE LYMPH NODES
Anatomical structure that defines the lymph node is the pectoralis minor.
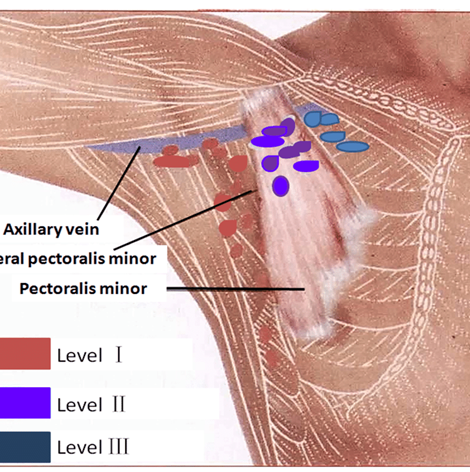
1. Level I (Low Axillary Nodes): Located lateral to the pectoralis minor muscle, closer to the arm. These are the first nodes to receive lymphatic drainage from the breast.
2. Level II (Mid Axillary Nodes): Situated deep to the pectoralis minor muscle, directly beneath it. They receive lymph from Level I nodes and are a secondary site for metastasis.
3. Level III (Apical Axillary Nodes): Located medial to the pectoralis minor muscle, near the subclavian vein. These nodes are involved in more advanced stages of cancer, receiving drainage from Levels I and II.
WHY is the lymphatic ducts removed ?
When DCIS is removed (like with a lumpectomy or mastectomy), nearby lymph nodes are often checked to see if cancer has spread beyond the ducts. This helps doctors understand how far the cancer has progressed and what treatments might be needed next.
Risk Assessment: Even though DCIS stays within the ducts, there’s a small chance that cancer cells could be in nearby lymph nodes. Removing and testing these nodes helps doctors decide on the best treatments, like radiation or hormone therapy, to prevent cancer from coming back.
Patient Care: Knowing if cancer cells are in the lymph nodes is important for planning the best care and predicting how the cancer might behave in the future. It helps doctors make decisions about treatment that can reduce the chances of cancer returning or spreading further.